When we first got the diagnosis of trisomy 18, and truly believed the predominant mythology that children with trisomy 18 are 'incompatible with life', Chris asked the fetal medicine consultant, "What do babies with trisomy 18 die of?" He got the answer that we would come to find everyone give: a shrug of the shoulders, a change of the subject, a "Well...trisomy 18," in a doubtful voice.
It seemed that nobody knew why children with trisomy 18 as a group tend to die prematurely. It seems to me that:
- It's an obvious question that parents of children with a new diagnosis will ask. So, if you're involved in communicating a diagnosis to parents, then you should have an answer.
- If you want to prevent premature death in children with trisomy 18, it might help to know what they're all dying of.
So what do children with trisomy 18 die of?
Here is a list of some of the most common causes of death:
- Placental insufficiency (common cause of stillbirth)
- Apnea (predominantly central)
- Respiratory insufficiency due to pulmonary hypoplasia, hypoventilation, airway obstruction or aspiration
- Cardiac failure
- Infection
You are likely now better informed than your geneticist, fetal medicine consultant, obstetrician, neonatologist and palliative care consultant! (If this is the case, give them a copy of Cereda and Carey for a basic T18 overview, in order to to further their professional education.)
You may find that, at some point, someone tells you that babies with T18 die because of 'changes at the cellular level'. We were told this very early on by a palliative care consultant and, after Rumer's death, by a pathologist. As far as I can discover, there is no research to support their claims, but it is an interesting theory which makes some sense. However, when it was used with us, I got the impression it was a more palatable substitute for, "We haven't a clue."
How can these risks be managed?
So now you know the common causes of death, you can work to prevent them.
- Good pregnancy management, including dopplers and frequent CTG monitoring, can minimise the risk of stillbirth.
 |
| Lots of CTGs! |
- Get your resuscitation skills up to date. Get a sats monitor and apnea monitor: detect apneas early and resuscitate appropriately. Central apneas are usually grown out of. All apneas should be investigated thoroughly to exclude obstructive causes and seizures.
 |
| EEG to investigate cause of apnea |
- Provide sufficient respiratory support to infants with pulmonary hypoplasia. Sadly some babies may have unsurvivable pulmonary hypoplasia, but many simply need time for their lungs to grow.
- If central hypoventilation (under-breathing) is an issue, discuss the possibility of trach-vent or other respiratory support at home. Most children, again, will grow out of it; some may not.
- Most children with T18 should have an MLB (microlaryngobronchoscopy) to exclude obstructive airway issues. They are the cause of approximately 40% of apneas in trisomy 18. Manage obstructive airway issues appropriately! Some children may benefit from nasopharyngeal airways or tracheostomy.
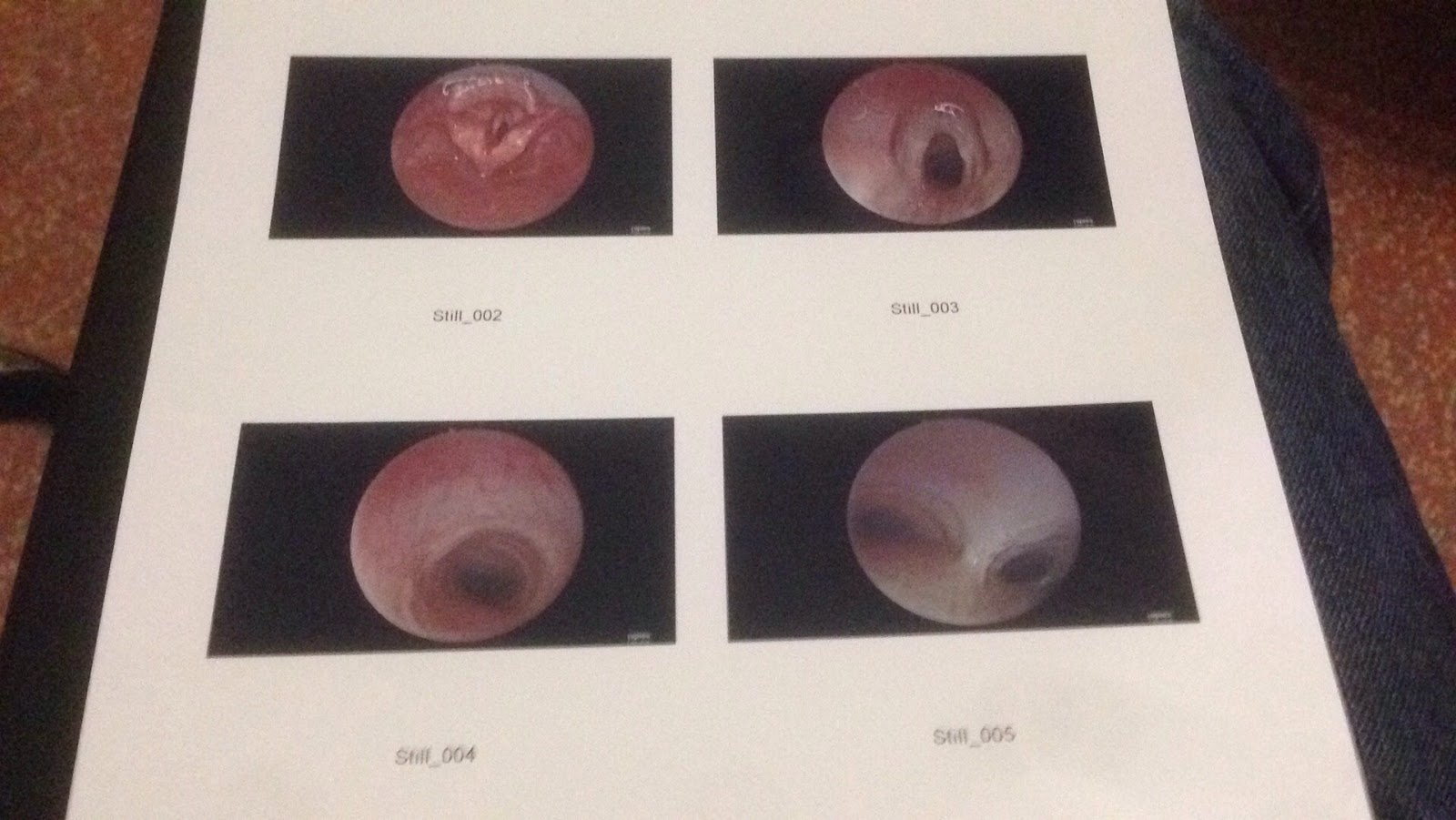 |
| Rumer's airways: views from the MLB |
- All children with T18 should have their swallow assessed and be fed in a way which minimises the risk of aspiration. Be clear with your SALT (Speech And Language Therapist) that you do not want to take even a low risk of aspiration. Suction may minimise aspiration of secretions for some children.
 |
| We tried this only once due to aspiration |
- Ensure cardiology are on board and are managing cardiac issues appropriately and early. A top question for cardiology, and for all doctors for that matter, is: "How would you manage a child without T18?"
- Vaccinate! Avoid exposure to infections wherever possible; try to stay out of hospital; arrange to come in only for needed treatment. All visitors must wash hands, and limit them strictly, especially in the winter. Fight for your baby to get the RSV vaccine. Get yourself, and any family and friends who help out, flu-vaccinated.
Can you completely avoid death? No. But if you can get appropriate management, you can increase the chances of your child being a longer-term survivor. You can see many of their pages here and here.
No comments:
Post a Comment
Comments appear with some delay to allow moderation. Thanks for commenting!